
15 de julho de 2019
A recorrência de dor lombar em um ano é comum? 69% das pessoas com dor lombar podem ter novos episódios em um ano, mas com poucas limitações.

Nas últimas semanas, me inspirei a aprofundar alguns dos mecanismos relacionados à atividade da “neurotag”, ou seja, a atividade das redes funcionais do cérebro envolvidas no processamento da dor. Tomando como base o brilhante Curso Explain Pain do Prof. Moseley em Copenhague, e o fascinante video TED “Your brain hallucinates your conscious reality (Seu cérebro alucina sua realidade consciente)” apresentado pelo neurocientista Anil Seth, tentei ter uma compreensão sobre dois tópicos em particular: o Processamento preditivo e a precisão interoceptiva. Eu não sou uma especialista nesse campo, e esses pensamentos ainda estão em progresso.
Em suma, o processamento preditivo é a melhor tentativa do cérebro de entender o mundo e resulta de tentativas de adaptar informações que se desviaram das nossas previsões (Clark, 2016). Agora sabemos que nossas experiências são inferidas (Heidegger, 1962; Sullivan, 1995); que costumamos preencher as lacunas (Gregory, 1980), que direcionameos a nossa atenção de maneira seletiva (Allport, 1993; Dayan et al, 2000; Beierholm et al, 2009; Howhy, 2012) e, em essência, priorizamos a eficiência com exatidão (Humphrey, 2005; Trimmer et al, 2013a). Para sobreviver, devemos perceber o nosso ambiente de forma eficaz, identificar ameaças e agir para evitar danos ao nosso corpo ou, se ocorrerem danos, devemos agir rapidamente para promover a recuperação (Tabor et al, 2017). Butler & Moseley (2013) e Trimmer et al. (2013b) descrevem que a dor, seja aguda ou crônica, é sempre racional, de acordo com o conjunto de informações disponíveis para a pessoa e como parte de uma estratégia de proteção. Esta perspectiva é congruente com a estrutura de inferência bayesiana (Edwards, 2012; Friston, 2011; Yuille et al, 2005) que enfatiza a importância de entender como a informação sobre o mundo, tanto interna quanto externa, está integrada na formação da experiência perceptual (Anchisi & Zanon, 2015; Yoshida et al, 2013). Uma análise precisa é crucial porque uma má compreensão das sensações como a dor pode resultar em decisões erradas sobre a causa da dor e, portanto, sobre a melhor ação a ser tomada (Tabor et al, 2017). Curiosamente, pode parecer que experiências que violam nossas previsões criam erros preditivos que levam a uma maior resposta protetora – uma resposta incorporada que ocorre fora de nossa consciência. Se isso é meramente relacionado às percepções da realidade, ou inclui a dor persistente, isso continua a ser objeto de estudo (o que eu sei até o momento).
Então, por que eu acho que a precisão interoceptiva pode ser importante para a dor?
A informação sobre o estado corporal é pertinente para fazer previsões, e de acordo com Clark et al (2015), a precisão interoceptiva é um processo preditivo que envolve “o uso do conhecimento adquirido para prever as informações sensoriais recebidas”. Mais importante ainda, a matriz interoceptiva coleta informações fisiológicas de todos os tecidos do corpo e diz respeito à homeostase ideal e ao bem-estar do organismo (Jänig, 2006). Di Lernia (2016) sugere que existe um elo perdido entre o sentido da condição fisiológica de todo o corpo e as percepções da dor em condições persistentes e que as teorias de codificação preditiva podem explicar um princípio subjacente de importância para a dor persistente. Di Lernia sugere ainda a existência de um “buffer antecipatório / interoceptivo” – um buffer que perde a sua relevância (sensibilidade) na dor persistente, o que representa uma hipótese interessante. Se esta linha de raciocínio é provável, isso pode implicar que somos menos sensíveis ao que está ocorrendo “aqui e agora”. Se olharmos para as teorias modernas da ciência da dor, como o “Modelo de Dor Neuromatrix de Melzack” (Melzack, 2005), sabemos que a dor como output depende de um tipo de mecanismo auto-referencial que se analisa de forma circular. A evidência empírica também sugere que há uma ponderação de precisão, que é um processo que acontece em todo o cérebro (Iglesias et al, 2013), e isso pode ser fundamentado através de mecanismos neuromoduladores em um nível sináptico (Moran et al, 2013; Seth & Friston, 2016). O equilíbrio entre os reflexos homoeostáticos e o comportamento alostático mais orientado para o objetivo depende da confiança (ou seja, da precisão) colocada em expectativas mais profundas sobre como nos comportaremos (Seth & Friston, 2016). Mais uma vez, se isso se aplica a dor persistente ainda precisa ser investigado com rigor.
Mas e se nossa capacidade de sentir nosso próprio estado corporal e processar essa informação é distorcida e não é tão precisa quanto antes? Todas as experiências e crenças anteriores sobre nosso próprio estado corporal não afetariam nossas previsões sobre o futuro? Então, e se nossas previsões causarem mais danos do que benefício?
Portanto, eu me pergunto se as intervenções terapêuticas que ajudam nossos pacientes são capazer de modificar com sucesso nosso modelo interno para fazer previsões precisas? Se a violação da expectativa do cérebro ocorre com a reconceptualização da crença e reduz os erros de predição, o que minimizaria a necessidade da proteção biológica ou psicossocial? Quando explicamos a dor e aumentamos a conscientização sobre DIMs (Danger in Me) e SIMs (Safety in Me), fornecemos conhecimento, recursos e capacitamos os pacientes – o que fornece ao paciente menos “coisas” para se preocupar, catastrofizar e ruminar. Se limitarmos o número de previsões disponíveis, podemos limitar a quantidade de erros de predição e, portanto, a necessidade de proteção em vários níveis. E se nós atualizarmos simultaneamente a precisão interoceptiva ou melhorar o “buffer antecipatório / interoceptivo” (criar propriedade do corpo, atenção / aceitação, melhorar a discriminação sensorial) – seria possível atualizar o modelo de predição, reduzindo os erros de previsão? Em termos mais amplos, isso significa que estamos buscando uma atividade de “neurotag”, deslocando o indicador para baixo no “protetômetro”? (Figura 1).
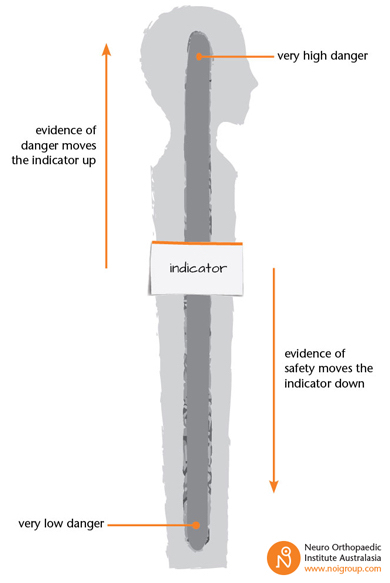
Figura 1. Protetômetro
Como nota final – precisamos ter uma perspectiva de sistemas que inclua conhecimento sobre neurofilosofia, o sistema nervoso, o sistema imunológico, o sistema endócrino e assim por diante. Estas são as “grandes rochas” que precisam ser exploradas antes de começar a focar nos pequenos grãos. O novo livro Explain Pain Supercharged gerencia eficazmente os pacientes em uma perspectiva de sistemas e, mais importante, em uma perspectiva biopsicossocial, e nos ensina a impulsionar nossas habilidades de comunicação e educação. Além disso, nos ensina a conceituar a dor persistente para os pacientes. Talvez a narrativa do paciente possa nos ajudar a entender como um indivíduo dá sentido ao mundo, e talvez mais pesquisas neste campo possam melhorar nossa compreensão entre ação e predição. No fim, a Revolução da dor é definitivamente necessária para mudar as crenças, o caminho no nível social e cultural, e as previsões individuais sobre nosso corpo e sobre o movimento.
In the last couple of weeks, I have been inspired to delve into some of the mechanisms related to “neurotag” activity – i.e. activity in functional networks that are involved in producing pain as an output. Both the light of Prof. Moseley’s brilliant Explain Pain Supercharged-course in Copenhagen, and the fascinating TED-talk “Your brain hallucinates your conscious reality” by neuroscientist Anil Seth, I’ve tried to get a grasp on two topics in particular: predictive processing and interoceptive accuracy. I am by no means an expert in the field, and these thoughts are work in progress so please proceed with a kind mind.
In short, predictive processing is the brain’s best attempt of making sense of the world, and results from attempts to accommodate information that has deviated from our predictions (Clark, 2016). We now know that our experiences are inferred (Heidegger, 1962; Sullivan, 1995); we fill in the gaps (Gregory, 1980), selectively attend (Allport, 1993; Dayan et al, 2000), unconsciously prime (Beierholm et al, 2009; Howhy, 2012), and in essence prioritize efficiency over accuracy (Humphrey, 2005; Trimmer et al, 2013a). In order to survive, we must perceive our environment effectively, identify threats, and act to avoid damage to our body – or, if damage occurs, we must act rapidly to promote recovery (Tabor et al, 2017). Butler & Moseley (2013), and Trimmer et al (2013b) argue that pain, whether acute or chronic, is always rational, according to the suite of information available to the person, and as part of a protective strategy; one attempts to defend one’s self in the presence of inferred threat (Wall, 1979). This perspective is congruent with the Bayesian inference framework (Edwards, 2012; Friston, 2011; Yuille et al, 2005) which emphasizes the importance of understanding how information about the world, both internal and external, is integrated in the formation of perceptual experience (Anchisi & Zanon, 2015; Yoshida et al, 2013). A precise and accurate analysis is crucial because a poor understanding of sensations like pain may result in erroneous decisions about the cause of pain and, therefore, about the best course of action (Tabor et al, 2017). Interestingly, it may seem that experiences that violate our predictions, i.e. unexpected ones, create predictive errors that lead to a greater protective response – an embodied response that occurs outside our awareness. Whether this is merely related to perceptions of reality, or includes persistent pain – remains to be validated (as far as I know).
So why do I think that interoceptive accuracy (or precision) may be important for pain? Information about the bodily state is pertinent to make predictions, and according to Clark et al (2015), interoception is a predictive process that involves “the use of acquired knowledge to predict the incoming sensory barrage”. More importantly, the interoceptive matrix collects physiological information from all tissues of the body and concerns optimal homeostasis and wellbeing of the organism (Jänig, 2006). I am not convinced that interoception has a superior role compared to proprioception or exteroception – but the literature is quite interesting. Di Lernia (2016) suggest that there is a missing link between the sense of the physiological condition of the entire body and the perceptions of pain in persistent conditions, and that predictive coding theories may explain an underlying principle of importance for persistent pain. Di Lernia further suggest the existence of an “anticipatory/interceptive buffer” – a buffer that loses its salience (sensitivity) in persistent pain, which represents an interesting hypothesis. If this line of reasoning is probable, it may imply that we are less responsive to what is occurring “here and now”. If we look at modern pain science theories such as Melzack’s “Pain Neuromatrix Model” (Melzack, 2005) or Gifford’s “Mature Organism Model” (Gifford, 1998) we know that pain as an output is dependent on a type of self-referential mechanism that samples itself in a circular manner. The Mature Organism Model suggests that pain can be considered an integrative experience forged upon sampling, appraisal, scrutinizing, and response processes from a top-down perspective. Empirical evidence also suggests that there is a precision-weighting, which is a generic computational process happening throughout the brain (Iglesias et al, 2013), and this may be instantiated through neuromodulatory mechanisms of gain control at a synaptic level (Moran et al, 2013; Seth & Friston, 2016). Importantly, the balance between homoeostatic reflexes and more goal-directed allostatic behaviour rests upon the confidence (i.e. precision) placed in deeper expectations about how we will behave (Seth & Friston, 2016). Again, whether this applies to persistent pain still has to be investigated rigorously. But what if our ability to feel our own bodily state, and to process that information is distorted and no longer as precise as it once were? Wouldn’t all prior experiences and beliefs about our own bodily state influence our predictions about the future? Thus, what if our predictions cause more harm than good?
Therefore, I wonder whether the therapeutic interventions that help our patients are the ones that successfully update our internal model for making precise predictions? Perhaps the top-down expectancy violation that occurs with belief reconceptualization reduces prediction errors, which then minimizes an existential need for biological or psychosocial protection (from an embodied first-person perspective)? When we explain pain and increase awareness of DIMs (Danger in Me) and SIMs (Safety in Me), we provide knowledge, resources and empower patients – which gives the patient less “stuff” to worry, catastrophize, and ruminate about. If we limit the number of predictions available to make, we may limit the amount of prediction errors, and thus, the need for protection on multiple levels throughout the hierarchy. What if we simultaneously update interoceptive accuracy or improve the “anticipatory/interoceptive buffer” (create body ownership, mindfulness/acceptance, improve sensory discrimination) – is it possible that we update the “sample and scrutinize”-model by reducing top-down and bottom-up prediction errors? In broader terms, does this mean that we are we targeting “neurotag” activity, shifting the indicator downwards on the “protectometer”? (Fig.1).
Fig.1: Protectometer (Butler & Moseley, 2017).
As a final note – we need to take a systems perspective that includes knowledge about neurophilosophy, the nervous system, the immune system, the endocrine system, gut-brain-axis, sleep hygiene, and so forth. These are the “big rocks” that needs to be put in the jar before we start focusing on the small grains. Explain Pain Supercharged effectively manages patients in a systems perspective, and importantly, in a biopsychosocial perspective, and teaches us to boost our communication and educational skills. Moreover, it teaches us to become brilliant belief “revisioners”/re-conceptualizers for patients with persistent pain. Perhaps the patient’s narrative may help us understand how an individual makes sense of the world, and perhaps more research in this field may improve our understanding between action and prediction. At the end of the day, the Pain Revolution is definitely needed to shift beliefs, all the way from a societal and cultural level, down to the individual predictions about our bodies and about movement that continue to create our reality.
References
Anchisi D., & Zanon M. A. (2015). Bayesian perspective on sensory and cognitive integration in pain perception and placebo analgesia. PLoS One, 10:e0117270.
Allport D.A. (1993). Attention and control: have we been asking the wrong questions? A critical review of twenty-five years. In: Meyer E, Kornblurn S, editors. Attention and performance XVI: synergies in experimental psychology, artificial intelligence, and cognitive neuroscience. Cambridge: MIT Press, p. 182–218
Barrett L.F., Simmons W.K. (2015). Interoceptive predictions in the brain. Nat Rev Neurosci, 16(7), 419-29.
Beierholm U.R., Quartz S.R., Shams L. (2009). Bayesian priors are encoded independently from likelihoods in human multisensory perception. J Vis, 9, 1–9.
Butler D.S., Moseley G.L. (2013). Explain Pain: Revised and Updated. Adelaide, Australia: Noigroup Publications
Butler D.S., & Moseley G.L. (2017). Explain Pain Supercharged. NOI group publications.
Clark A. (2015). Radical predictive processing. South J Philos. 53, 3–27.
Clark A. (2016). Busting out: predictive brains, embodied minds, and the puzzle of the evidentiary veil. Nous, 1–27
Di Lernia D., et al. (2016). Ghosts in the Machine. Interoceptive Modeling for Chronic Pain Treatment. Front Neurosci, 10, 314.
Dayan P., Kakade S., Montague P.R. (2000). Learning and selective attention. Nat Neurosci, 3, 1218–23.
Edwards M.J., Adams R.A., Brown H., et al. (2012). A Bayesian account of ‘hysteria’. Brain, 135, 3495–3512.
Friston K. (2011). Embodied inference: or I think therefore I am, if I am what I think. In: Wolfgang T, Bergomi C, eds. The Implications of Embodiment (Cognition and Communication). Exeter: Imprint Academic, p. 89–125.
Gregory RL. (1980). Perceptions as hypotheses. Philos Trans R Soc B Biol Sci, 290, 181–97.
Gi?ord, L. S. (1998). “The mature organism model,” in Topical Issues in Pain. Whiplash – Science and Management. Fear-Avoidance Beliefs and Behaviour, ed L. S. Gi?ord (Falmouth: CNS Press), p. 45–56.
Heidegger M. (1962). Being and time. (Macquarrie J, Robinson E, translater/editor). Tubingen: Max Niemeyer Verlag.
Hohwy J. (2012). Attention and conscious perception in the hypothesis testing brain. Front Psychol, 2, 96.
Humphrey N. (2005). The placebo effect. In: Gregory R, editor. Oxford companion to the mind. Oxford: Oxford University Press.
Iglesias S., et al. (2013). Hierarchical prediction errors in midbrain and basal forebrain during sensory learning. Neuron, 80, 519-530.
Jänig, W. (2006). The Integrative Action of the Autonomic Nervous System: Neurobiology of Homeostasis. Cambridge; New York, NY: Cambridge University Press. doi: 10.1017/CBO9780511541667
Melzack, R. (2005). Evolution of the neuromatrix theory of pain. The Prithvi Raj Lecture: presented at the third World Congress of World Institute of Pain, Barcelona 2004. Pain Pract. 5, 85–94.
Moran R.J., et al (2013). Free energy, precision and learning: the role of cholinergic neuromodulation. J Neurosci, 33, 8227-8236.
Seth A., Friston K. (2016). Active interoceptive inference and the emotional brain. Philos Trans R Soc Lond B Biol Sci, 371(1708).
Sullivan M.D. (1995). Pain in language from sentience to sapience. J Pain, 4, 3–14.
Tabor A., et al (2016). Perceptual inference in chronic pain. An investigation into the economy of action hypothesis. Clin J Pain, 32(7), 588-93.
Tabor A., et al. (2017). Pain: A statistical account. PLOS Computational Biology, 13(1), e1005142.
Talsma, D. (2015). Predictive coding and multisensory integration: an attentional account of the multisensory mind. Front Integr Neurosci, 9, 19.
Thacker, M. (2015). Louis Gi?ord – revolutionary: the Mature Organism Model, an embodied cognitive perspective of pain. Psychother Priv Pract, 152, 4–9.
Trimmer P.C., et al. (2013a). Understanding the placebo effect from an evolutionary perspective. Evol Hum Behav, 34, 8–15.
Trimmer P.C., et al. (2013b). On the evolution and optimality of mood states. Behav Sci, 3, 501–521.
Yoshida W., Seymour B., Koltzenburg M., et al. (2013). Uncertainty increases pain: evidence for a novel mechanism of pain modulation involving the periaqueductal gray. J Neurosci, 33, 5638–5646.
Yuille A., Kersten D. (2006). Vision as Bayesian inference: analysis by synthesis. Trends Cogn Sci, 10, 301–308.
Wall P.D. (1979). On the relation of injury to pain. The John J. Bonica Lecture. Pain, 6(3), 253–64.









Leave a comment